

Torticollis
Torticollis is caused by stiffness or shortening of a neck muscle (the sternocleidomastoid – SCM). The baby then keeps their head tilted to one side and turned to the other. Torticollis is present at birth and often noticed in the first days or weeks of life.
Common symptoms: how to recognize torticollis?
A baby may have torticollis if you notice one or more of the following:
- Your baby always sleeps with their head turned to the same side;
- If you try to turn your baby’s head to one side, but they always bring it back to the other side;
- Your baby often keeps their head tilted to one side (the distance between the ear and shoulder is reduced on one side compared to the other) when lying on their back, on their tummy, and/or sitting, and they cannot keep it centered;
- On one side, the baby can fully turn their head and rest their cheek on the mattress. On the other side, instead of resting the cheek down, they cannot turn their head completely and may even turn their whole body instead of just the head.
Flat head
Why can my baby’s head become flat?
The recommendation for babies to sleep on their backs has significantly reduced the risk of sudden infant death syndrome. This positioning remains essential, but it also means babies spend long hours with the back of their head resting on the mattress. If a baby keeps their head in one position more often than another, this can contribute to plagiocephaly (flat head). Even when awake, babies under 4 months often spend a lot of time on their backs, especially if they do not enjoy tummy time.
The malleability of the skull bones, their separation, and the rapid skull growth between 0 and 4 months are the main factors contributing to possible flattening.
What is flat head syndrome? Two types of flattening
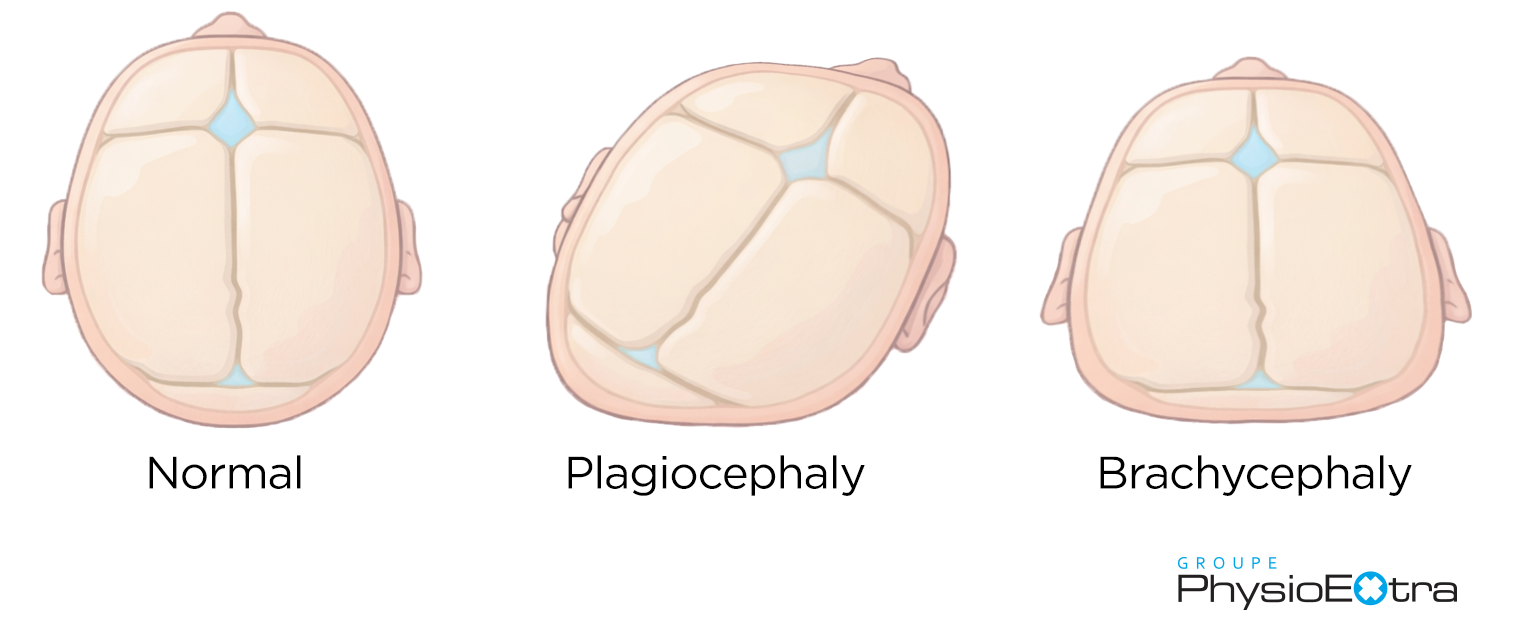
Plagiocephaly is flattening on one side at the back of the baby’s head, caused by prolonged pressure on the same area.
Causes: This is mainly due to congenital torticollis, which keeps the head turned more to one side. Plagiocephaly may also result from the baby’s preferred position in the womb (especially late in pregnancy or in multiple pregnancies) or from a natural preference to turn the head to the same side, especially at night. Daily habits can also play a role—for example, always interacting with the baby from the same side.
Brachycephaly is symmetrical flattening across the back of the skull.
Causes: It mostly occurs when a baby keeps their head centered during sleep (even though gravity should naturally tilt the head to one side or the other) and spends a lot of time on their back with limited tummy time. A baby with higher muscle tone who frequently pushes into extension may also be more likely to develop brachycephaly.
Is it serious?
These deformities are often mild but can become severe in as little as 3–4 weeks if not addressed. They occur due to the skull’s high malleability (useful during birth) and the rapid skull growth between 0 and 4 months. Skull growth slows around 4 months, although it continues. By age 2, major skull growth is nearly complete.
When should you stop worrying about flat head?
Rest assured, once your baby can roll independently, sit, and has not developed flat head by around 6 months, the likelihood of plagiocephaly or brachycephaly developing is very low. A deformity requires prolonged head pressure on a surface such as a cushion, a parent, or the floor.
And if the deformity persists?
Around 5–6 months, if progress is limited and plagiocephaly/brachycephaly is more significant, the family doctor may refer the baby to a physiatrist. They will assess whether a cranial orthosis (helmet) is needed. The helmet is typically worn 23 hours a day for 8–12 weeks. Rest assured: the helmet is usually more unsettling for parents than for the baby, who generally tolerates it very well.
Because the orthosis cannot be used once the sutures begin to close (around 12–18 months), early intervention is essential to avoid permanent deformation.

When should you consult?
As soon as you notice early flattening, a preference for head rotation, or a baby who keeps their head tilted to one side. The earlier babies are seen (ideally within the first months of life), the faster the recovery and the less impact on motor development. After 4 months, the skull becomes less malleable and grows more slowly, making therapy results harder to achieve.
Take time to observe your baby and notice whether they consistently hold their head on the same side or if the shape of their skull has changed. If in doubt, it is important to consult quickly in physiotherapy or osteopathy, ideally with pediatric expertise. Discuss it with your doctor as well.
YOU
KNOW?
A medical referral is not required to book a physiotherapy appointment for your baby.
Physiotherapy or osteopathy?
Both approaches are effective and complementary but must be combined with good home habits and playful exercises to enhance treatment.
- Physiotherapy aims to improve mobility, reinforce symmetry, and stimulate motor development through exercises, stretches, and positioning strategies. Parents play a central role, and exercises will be provided to continue the work at home.
- Osteopathy focuses on the mobility of cranial sutures and reducing tension.
At PhysioExtra, babies are first assessed in physiotherapy. If needed, the physiotherapist may recommend osteopathy to complement treatment.
What are the possible long-term impacts?
Rest assured: head shape has no effect on a child’s intellectual abilities. However, torticollis or plagiocephaly/brachycephaly can affect motor development. A baby who always turns their head to the same side may become stronger and more skilled on one side. You may notice:
- more frequent use of one hand;
- rolling, pivoting, or transitions always performed on the same side;
- a tendency to pull up to stand using the same leg.
Skull asymmetry may also have aesthetic impacts: visible flattening, a more prominent forehead, asymmetry of the eyes or ears, difficulty wearing glasses, hats, or bike helmets, and sometimes mild effects on dental occlusion.
How to prevent it?
- Stimulate your baby equally on both sides to avoid head flattening during sleep and awake time.
- Avoid letting your baby develop the habit of sleeping with their head centered without rotation.
- Encourage your baby to spend time on the floor on a playmat from birth and limit long periods in swings, car seats, and other seats. This allows more head movement and reduces flattening.
However, congenital torticollis cannot be prevented, as it results from external and uncontrollable factors. It is therefore essential to consult to determine whether the head-turning preference is simply habitual or true torticollis.
Simple little tips
During feeding
Alternate sides when breastfeeding or bottle-feeding.
During naps
Change your baby’s head position: one time to the right, then to the left. Avoid positioning pillows. Under supervision, your baby can also nap on their side or in a baby carrier.
During nighttime sleep
Always place your baby on their back. Alternate the direction of their head in the crib each night to encourage rotation to both sides. Snuggle Me–type mattresses and any other crib add-ons are not recommended during unsupervised nighttime sleep.
During playtime
Place your baby on their tummy for short periods from the first days. You can also place them on your chest or use a small cushion under their chest. Vary your position so your baby looks to the right, left, and center.
When out for a walk
Prefer a bassinet-style stroller (which allows more freedom of head movement) or a baby carrier rather than keeping the car seat attached to the stroller.
To avoid
Long periods in the car seat and seats that keep the head centered, as they increase pressure on the back of the head.
So, should you worry?
There is no medical reason for concern, but it is important to consult early, ideally within the first month. Earlier intervention leads to faster and more complete results.
Plagiocephaly and torticollis do not resolve on their own: a physiotherapy assessment will help support your baby toward symmetrical and healthy development.




